
On August 9, 2018, the Centers for Medicare and Medicaid Services (CMS) issued a proposed rule to overhaul the Medicare Shared Savings Program (MSSP). The proposal, titled "Pathways to Success," would make significant changes to the accountable care organization (ACO) model at the heart of the program. The proposed changes include a restructuring of the current ACO risk tracks, updating spending benchmarks, increased ACO flexibility to provide care, as well as changes to the electronic health records requirements for ACO practitioners.
Background
There are currently 561 Shared Savings Program ACOs serving over 10.5 million Medicare fee-for-service (FFS) beneficiaries. Under the MSSP, ACOs are assessed based on quality and outcome measures, and by comparing their overall health care spending to a historical benchmark. ACOs receive a share of any savings under the historical benchmark if they meet the quality performance requirements.
Currently, the MSSP allows ACOs to participate in one of three "tracks." Track 1 is a "one-sided" model, meaning that participating ACOs share in their savings, but are not required to pay back spending over the historical benchmark. Track 2 and Track 3 are "two-sided" models, meaning that participating ACOs share in a larger portion of any savings under their benchmark, but may also be required to share losses if spending exceeds the benchmark. Currently, the vast majority of ACOs participate in Track 1.
Restructuring the Tracks
CMS proposes retiring Track 1 and Track 2, creating a BASIC track, and renaming Track 3 the ENHANCED Track. CMS describes the BASIC track as a "glide path" that will help ACOs transition to higher levels of risk and potential reward. To that end, the BASIC track contains five levels that ACOs would transition through over the course of a five year contract period, spending a maximum of one year at each level. The first two years would involve upside-only risk, with a transition to increasing levels of financial risk in the remaining three years. Current Track 1 ACOs will be limited to one-year of upside-only participation before taking on downside risk. This is a substantial acceleration from the current Track 1 Model, which permits ACOs to avoid downside risk for up to six years.
Finally, the proposed rule draws a distinction between low revenue ACOs and high revenue ACOs. Low revenue ACOs (typically composed of rural ACOs and physician practices) would be permitted to spend two 5-year contract periods on the BASIC track. High revenue ACOs (typically composed of hospitals) would be permitted only one 5-year contract period on the Basic track.
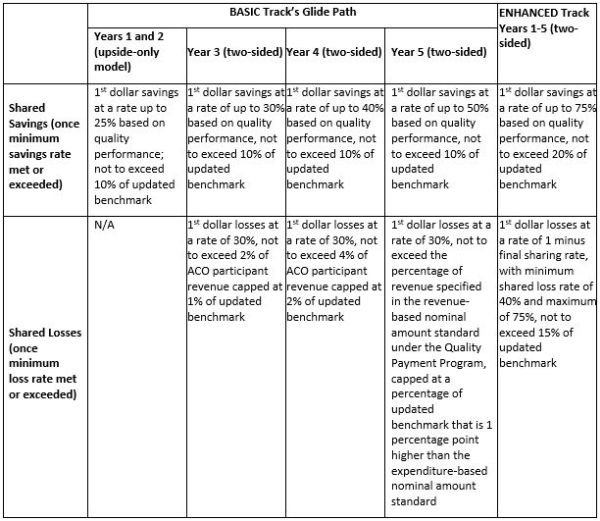
Source: Proposed Rule: Medicare Program; Medicare Shared Savings Program; Accountable Care Organizations–Pathways to Success
Updating the Historical Spending Benchmarks
Every year, an ACO's spending is comparing to its historical benchmark to determine the ACO's participation in any shared savings or losses. Under the proposed rule, the benchmark methodology will incorporate regional FFS expenditures beginning in the first contract period. Also, the historical benchmark will be rebased at the beginning of each 5-year contract period. Adjustments to the benchmark related to regional expenditures will be capped at 5% of the national Medicare FFS per capita expenditure. According to CMS, these changes will improve the predictability of historical benchmark setting and increase the opportunity for ACOs to achieve savings against the historical benchmark.
Expanding ACO Flexibility in Beneficiary Care
The proposed rule contains several changes to the MSSP aimed at increasing the flexibility of ACOs to provide cost-effective care to their assigned beneficiaries. For example, to support the ACO's coordination of care across health care settings, ACOs will be eligible to receive payment for telehealth services furnished to prospectively assigned beneficiaries even when they would otherwise be prohibited based on geographic prerequisites. The proposed rule also expands the Skilled Nursing Facility (SNF) 3-Day Rule Waiver to all ACOs in two-sided models. This waiver permits Medicare coverage of certain SNF services that are not preceded by a qualifying 3-day inpatient hospital stay.
Finally, the proposed rule permits ACOs in two-sided models to reward beneficiaries with incentive payments of up to $20 for primary care services received from ACO professionals, Federally Qualified Health Centers, or Rural Health Clinics.
Changing Electronic Health Record Requirements
Currently, one of the quality measures for which ACOs are assessed relates to the percentage of participating primary care providers that successfully demonstrate meaningful use of an electronic health records system for each year of participation in the program. The proposed rule eliminates this measure. Instead, CMS proposes to adopt an "interoperability criterion" that assesses the use of certified electronic health record technology for initial program participation and as part of each ACO's annual certification of compliance with program requirements.
Commentary
CMS's proposal is not surprising in light of CMS Administrator Seema Verma's recent comments about upside-only ACOs. At an American Hospital Association annual membership meeting this past spring, Administrator Verma is quoted as saying:
[T]he majority of ACOs, while receiving many waivers of federal rules and requirements, have yet to move to any downside risk. And even more concerning, these ACOs are increasing Medicare spending, and the presence of these 'upside-only' tracks may be encouraging consolidation in the market place, reducing competition and choice for our beneficiaries. While we understand that systems need time to adjust, our system cannot afford to continue with models that are not producing results.
Though the rule is only a proposal at this time, the above comments illustrate that CMS is serious about requiring providers to be more financially accountable for the care of their patients. And the agency is clear-eyed about the short-term impact of the proposal, estimating that more than 100 ACOs will exit the MSSP over the next 10 years if the proposal is finalized. The agency nevertheless believes that the new program would be attractive to providers due to its simplicity (as compared to the current program) and the new opportunity it offers clinicians to qualify as participating in an Advanced Alternative Payment Model (APM) when they reach year 5 of the BASIC track. APMs are an important concept under the Quality Payment Program (QPP) that was ushered in by the Medicare Access and CHIP Reauthorization Act of 2015. Clinicians participating in an Advanced APM are exempt from reporting under the QPP's Merit-based Incentive Payment System (MIPS) and are eligible for certain financial incentives. The fates of the MSSP and the QPP are thus intertwined, and the co-evolution of the programs is at a critical stage, especially in light of CMS's July release of a proposed rule modifying the QPP. We will continue to report on the developments of both of these programs.
Those interested in commenting on the MSSP proposal must do so by October 16, 2018.


